Next Steps
Is the intervention sustained locally after education and training?
Our prior research has shown that removing aquatic vegetation from water access points removes snail habitat, thereby reducing both snail populations and human schistosomiasis prevalence, while increasing access to water for cooking and washing. The next step is to sustain vegetation removal in the absence of westerner assistance. But poor communities' governments lack fiscal resources to provide this essential public good. They must motivate private individuals to provide the public good: vegetation clearing for infectious disease control. How? And with what feedback effects in the socio-ecological system?
The next stage in this project is to disrupt the widespread reinforcing feedback between poverty and infectious disease by educating villagers on the public health and private benefits of waterway clearing that can control schistosomiasis, sustain ample open water and food supplies, and foster economic development. After baseline data collection, ¼ of 88 recruited communities in Senegal will be educated on the public (reduced schistosomiasis and increased open water access) and private benefits (increased food production and cooking gas and reduced costs on livestock feed) of the innovation, ¼ will only receive education on the public benefits, ¼ will only receive education on the private benefits, and the last ¼ will receive no education at all. We will then track in each community the amount of submerged aquatic vegetation, snails, and parasites in their water access points, quality of life and wealth, and spread of the knowledge within the communities. This study may offer a prototype for how to i) disrupt poverty disease traps, ii) synergistically integrate socioeconomic and environmental systems, iii) enhance public goods provisioning through activation of people’s pro-social preferences and/or private economic incentives, and iv) design and test incentives to sustain community-led maintenance of public goods.
Testing the intervention in other parts of Africa
In clinical trials in Senegal, removal of submerged aquatic vegetation from water access points reduced the human disease schistosomiasis and snails that transmit Schistosoma parasites to humans. However, aquatic ecology in Africa is heterogeneous, indicating that this innovation needs to be tested in other parts of Africa. For example, the dominant aquatic vegetation in Senegal is Ceratophyllum demersum, whereas the dominant aquatic vegetation on Lake Victoria in eastern Africa is invasive water hyacinth (WH, Fig. 1).
 Fig. 1. Invasive water hyacinth on Lake Victoria for kilometers in all directions.
Fig. 1. Invasive water hyacinth on Lake Victoria for kilometers in all directions.
The literature suggests a positive relationship between WH and snails, but a relationship between WH and schistosomiasis prevalence in humans has never been explored. By using historic data on schistosomiasis reinfection rates in villages on Lake Victoria and local WH levels the year before (using satellite imagery), we discovered that this relationship is hump-shaped, with prevalence increasing up to intermediate WH densities and then decreasing thereafter. We hypothesize that snail and cercarial (parasite stage that infects humans) densities are associated positively with WH densities but that human contact with the water is associated negatively, accounting for the hump-shaped relationship. We also hypothesize that humans shift from use of the Lake to inland waterbodies (streams and ponds) when WH is abundant.
To test these hypotheses, we are collaborating with Drs. Erick Muok and Maurice Odiere at the Kenyan Medical Research Institutes’ Center for Global Health Research in Kisumu to quantify snail and cercarial densities and human contact with the water across a gradient of WH levels at 20 water access points on Lake Victoria near Kisumu and at 20 nearby inland waterbodies (Fig. 2).
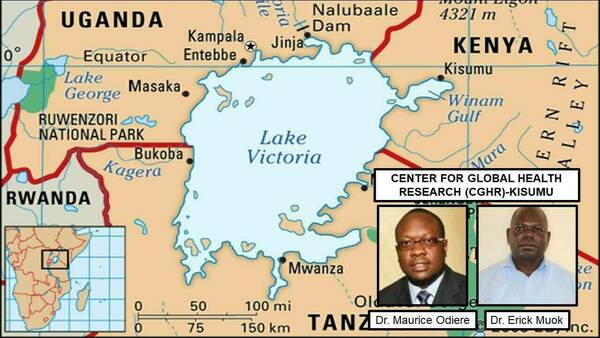 Fig. 2. Collaborators and location of water hyacinth-schistosomiasis work in Kenya.
Fig. 2. Collaborators and location of water hyacinth-schistosomiasis work in Kenya.
Snail, vegetation, and cercarial (parasite stage that infects humans) densities will be quantified. Human water use will be quantified by counting the number of humans in the water and the extent and duration of their water contact. Finally, to assess how and why human behavior is affected by varying WH levels, we will implement a sociological survey in these same villages. We hope this study elucidates the mechanisms driving the hump-shaped relationship between WH densities and schistosomiasis prevalence so we can effectively devise an intervention to improve health, such as aquatic vegetation removal that was effective in Senegal.